Keywords: lower limb rehabilitation; postoperative rehabilitation; NASA Anti Gravity Treadmill
Abstract
Objective To observe the effect of anti-gravity treadmill system in rehabilitation treatment after open reduction and internal fixation of femoral condylar fracture. Methods A total of 54 patients with femoral condylar fracture who underwent open reduction and internal fixation from June 2018 to June 2020 were enrolled. 27 patients received conventional rehabilitation combined with anti-gravity treadmill system training (observation group), and 27 patients received conventional rehabilitation after surgery (control group). The fracture healing time, time to recover full weight-bearing walking, gait recovery, and knee joint function at the last follow-up were compared between the two groups. Results All 54 cases were followed up for 6 to 18 months, with a median time of 12 months. The fracture healing time and time to recover full weight-bearing walking in the observation group were 14 weeks. The fracture healing time and time to recover full weight-bearing walking in the control group were 16 weeks. The fracture healing time and time to recover full weight-bearing walking in the observation group were significantly shorter than those in the control group, with statistically significant differences. The gait score of the observation group was 10 points after 20 weeks of treatment, which was better than 8 points in the control group, with statistically significant differences. At the last follow-up, the function, muscle strength and stability scores of the knee HSS score in the observation group were higher than those in the control group, and the difference was statistically significant; while there was no statistically significant difference in the pain, range of motion and knee flexion deformity scores between the two groups. Conclusion Anti-gravity treadmill system training can promote fracture healing in the early rehabilitation treatment after open reduction and internal fixation of femoral condylar fractures, and patients can walk with full weight-bearing earlier, and their gait recovers well, and finally obtain better knee function, muscle strength and stability.
General information Inclusion criteria: ①Age 20-60 years old, good physical fitness in the past; ②According to the diagnosis and treatment standards of femoral condyle fracture in the “Clinical Diagnosis and Treatment Guidelines·Orthopedics” and “Bone and Joint Injury”. It was diagnosed as unilateral closed femoral condyle fracture; ③Open reduction and internal fixation surgery was used for treatment, and the patient and his family members were informed and agreed to the surgical plan; ④The patient’s compliance was strong and cooperated with the treatment and follow-up; ⑤The study was approved by the hospital ethics committee. Exclusion criteria: ①Fractures in other parts of the affected limb or fractures of the contralateral lower limb; ②Combined with neurovascular injury and deep vein thrombosis of the lower limb; ③Combined with serious organ and hematopoietic system diseases; ④Local infection or abscess, weak constitution, combined with malignant tumors or cachexia. 54 cases were included, 27 cases received conventional rehabilitation combined with anti-gravity treadmill system training (observation group), and 27 cases received conventional rehabilitation treatment after surgery (control group). There were 19 males and 8 females in the observation group, aged 48 years old; fractures were classified according to AO: 10 cases of type A, 10 cases of type B, and 7 cases of type C. The control group included 18 males and 9 females, aged 47 years old. According to AO classification, there were 10 cases of type A, 9 cases of type B, and 8 cases of type C. There was no statistically significant difference in gender, age, and fracture type between the two groups.
Treatment methods: Open reduction and plate internal fixation surgeries were all performed by the same group of surgeons, and the specific surgical procedures are omitted. Routine postoperative treatment was performed, and drugs for promoting blood circulation and removing blood stasis, reducing swelling and relieving pain, and repairing tendons and bones were given according to the three-stage healing stage of the fracture. Routine rehabilitation training: ① Rehabilitation intervention was performed on the first day after surgery. The patient raised the distal limb of the affected side, and medium-frequency pulse electricity, local cold compress, lower limb air pressure and other treatments were given to promote swelling of the affected limb and prevent thrombosis; ② In the early stage (0-2 weeks after surgery), the patient was guided to perform toe activities and ankle pump training, isometric contraction of the quadriceps and gluteus maximus, straight leg raising training, and passive flexion and extension training of the knee joint (starting from 1 week after surgery, the range of motion starts from 0°~30° and gradually increases), and the patient was encouraged to perform active flexion and extension training of the knee joint in the largest possible range; ③ In the mid-term (3-6 weeks), passive flexion and extension training of the knee joint was continued, the continuous passive training angle was increased, the active training gradually increased the strength and amplitude, and the lower limb isometric and isotonic training was increased. The strength of each training To achieve the maximum range; perform patellar loosening training, the patient grasps the upper and lower poles of the patella with the thumb and index finger and pushes up and down and left and right to loosen the tissues around the patella, encourage and guide the patient to perform posture training such as sitting beside the bed with legs hanging down and hugging legs to increase the range of joint movement; ④ In the later period (after 6 weeks), X-rays are taken to review the fracture alignment and healing status, and partial weight-bearing training with crutches is started, and the weight of partial weight-bearing is gradually increased; strengthen the muscles around the knee joint and quadriceps muscle strength training, including leg hook exercises and resistance flexion and extension training, and gradually increase from rubber band resistance to sandbag resistance training; gradually perform full weight-bearing walking training without crutches, increase walking distance and frequency, and balance training after the patient is fully weight-bearing. In the later period, static squat training and stair climbing and descending training can be performed. The observation group used the anti-gravity treadmill system for weight-loss gait training on the basis of conventional rehabilitation training. The initial weight loss was 80%-90% of body weight, and the walking speed was 0.1m/s, twice a day, 20min each time; during training, the patients held the handrails with both hands to prevent the body from swaying, and the lower limb weight was increased by 8%-10% each week. The walking speed was gradually increased and the treatment time was gradually increased until full weight bearing. The control group only performed conventional rehabilitation training.
research results
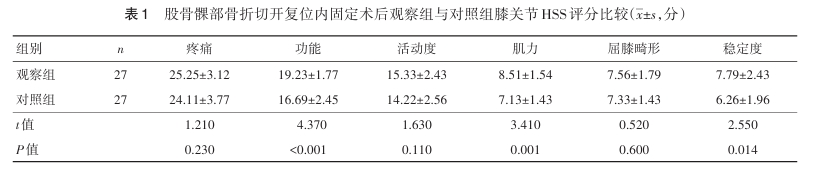
All 54 cases were followed up for 6 to 18 months, with a median of 12 months. During the follow-up period, no complications such as deep vein thrombosis, infection, nonunion of fracture, and failure of internal fixation occurred in all patients. The fracture healing time in the observation group was 14 weeks, and the time to recover full weight-bearing walking was 14 weeks. The fracture healing time in the control group was 16 weeks, and the time to recover full weight-bearing walking was 16 weeks. The fracture healing time and the time to recover full weight-bearing walking in the observation group were significantly shorter than those in the control group, and the differences were statistically significant. The gait score of the observation group was 10 points after 20 weeks of treatment, and that of the control group was 8 points; the gait score of the observation group was higher than that of the control group after 20 weeks of treatment, and the difference was statistically significant. At the last follow-up, the function, muscle strength, and stability scores of the knee HSS score in the observation group were higher than those in the control group, and the difference was statistically significant; however, there was no statistically significant difference in the pain, range of motion, and knee flexion deformity scores between the two groups.
In summary, the use of anti-gravity treadmill system training in early rehabilitation treatment after open reduction and internal fixation of femoral condylar fractures can promote fracture healing, and patients can walk with full weight earlier, with good gait recovery, and ultimately obtain better knee joint function, muscle strength, and stability.