Key words: Anti-gravity treadmill, Cadence, Running
Background
Running cadence, or step rate, is often measured in running gait analysis and manipulated in gait retraining. A lower body positive pressure treadmill, or anti-gravity treadmill, allows users to walk/run in a reduced gravity environment.
Purpose
The primary purpose of this study was to determine how natural running cadence is affected by running on an anti-gravity treadmill compared to a standard treadmill in a healthy, active population. The secondary purpose was to determine if natural and increased cadence is affected by amount of body weight support.
Study Design
Cross-sectional study (convenience sample).
Methods
Thirty participants were recruited to run on an anti-gravity treadmill ( Anti-Gravity TreadmillTM M320) at their pre-determined, self-selected, comfortable treadmill speed. Cadence was recorded at nine randomized bodyweight conditions, ranging from 100% of body weight to 20% of body weight, in 10% increments. An additional nine participants were recruited to try to replicate their natural, standard treadmill cadence, as well as increase it by 5% and 10%, while on an anti-gravity treadmill with the same randomized body weight conditions.
Results
Thirty participants, 19 females and 11 males, mean age 27.3 years (range, 22-45), completed Part 1 of the study protocol, while nine additional participants (2 females and 7 males) with a mean age of 29.6 years old (range, 25-40 years) completed Part 2 of the protocol. There was a significant effect of natural running cadence on the anti-gravity treadmill at reduced body weight percentages (p<.01). Post-hoc t-tests revealed that every 10% bodyweight interval was significantly lower than the previous 10% interval (p<.01) on the anti-gravity treadmill, with cadence decreases ranging from 1.5%-3.5% between intervals. Seven of the nine (77.8%) participants in Part 2 were able to replicate and increase their cadence at all body weight levels on the anti-gravity treadmill.
Conclusions
Decreasing bodyweight level on an anti-gravity treadmill yields a significant and linear decrease in running cadence when performed at a self-selected, moderate intensity pace. Further, the vast majority of participants were able to successfully replicate and increase cadence at all levels of bodyweight percentage.
Article cited in:Josie Stockland, PT, DPT,1 M. Russell Giveans, PhD, 1 and Peter Ames, PT, PhD1
1 and Peter Ames, PT, PhD1
Article link:THE EFFECT OF AN ANTI-GRAVITY TREADMILL ON RUNNING CADENCE
The recreational sport of running is associated with a high risk of overuse injury.1- The reported lower extremity injury rate ranges from 18% to 94%, with the greatest percentage of injuries being related to the knee. During a period of injury rehabilitation and potential reduction in running tolerance, runners often utilize cross-training modalities such as elliptical training or pool-related activities to supplement for or replace the aerobic benefits of running. Running step rate, or cadence, is routinely assessed in running gait analysis. Previous research supports the use of step rate manipulation through increased cadence to alter running kinetics and kinematics. Heiderscheit et al. demonstrated that an increase of 5% above natural running cadence reduces hip and knee joint loading, which may correlate with injury prevention and treatment of overuse injuries. Allen et al. found a step rate 10% above natural cadence was effective in transitioning those with a heel strike running pattern at initial contact to a non-heel strike or less severe heel strike pattern, altering ground reaction forces. An anti-gravity treadmill allows users to walk or run in a reduced body weight environment. The user walks or runs on a treadmill belt surrounded by an enclosed, air-filled chamber. When air pressure increases, an upward force offloads the weight of the runner and decreases the percentage of body weight (BW%) experienced upon foot impact. Anti-gravity treadmills provide a mode of aerobic exercise that impart reduced ground reaction forces and are utilized in the rehabilitation community as well as in the healthy population. Differences have been documented in both level of exertion and running mechanics between standard treadmill and anti-gravity treadmill running. Figueroa et al. determined that, in healthy subjects, the metabolic cost of running was less on an antigravity treadmill with body weight support as compared to a standard treadmill. Kline et al. published metabolic conversions for standard treadmill speeds compared to anti-gravity treadmill at 50% to 100% body weight support.
Two studies have investigated the effect of antigravity treadmill on running cadence. Raffalt et al.measured step length and frequency at five standardized speeds and at four BW% conditions on the antigravity treadmill in elite or sub-elite male runners. Across all speed intervals, as body weight support increased, step frequency decreased and step length increased. Neal et al. studied lower body kinematics in healthy male runners at three conditions equivalent to 60%, 70%, and 80% VO2 peak capacity. On the anti-gravity treadmill, ankle and knee kinematics were significantly altered during stance phase as compared to standard treadmill, and stance time significantly decreased when body weight was less than 80%. Spatiotemporal data collection in the previously mentioned studies was completed with in- shoe plantar pressure sensors. To the authors’ knowledge, no previous studies have investigated the effect of anti-gravity treadmill in a non-runner population or while allowing participants to use a self-selected pace. The primary purpose of this study was to determine how natural running cadence is affected by running on an anti-gravity treadmill compared to a standard treadmill in a healthy, active population. The secondary purpose was to determine if natural and increased cadence is affected by amount of body weight support. The authors hypothesized that: a) natural cadence would decrease on an anti-gravity treadmill compared to a standard treadmill, b) natural cadence would decrease with increasing body weight support on the anti-gravity treadmill, and c) over ground running cadence would be maintained through 50% of bodyweight, after which time it would no longer be feasible to maintain, and a 10% increase in step rate would be maintained through 60% of body weight.
.104-1-1024x689.png)
A sample of convenience participated in this study at a private, outpatient, physical therapy clinic. Participants were recruited through word of mouth via colleagues within a single institution. Inclusion criteria for participation included being between the ages of 18-49 being self-described as physically active (engaged in a regular activity regimen of >150 minutes of moderate intensity exercise causing perspiration or heavy breathing for sessions of 30 consecutive minutes or greater per week). Participants were also novice runners, performing lessthan 15 miles of running per week. Participants were excluded if they had sustained a lower extremity injury in the prior three months, had a history of lower extremity surgery, had a current back or lower extremity pain with running, had cardiovascular or neurological compromise, or were unable to provide voluntary consent.
Part 1: Participants performed a five-minute warm up on the standard treadmill; they were blinded to speed and instructed to increase the belt speed to a “moderate-intensity pace that you would run three miles or five kilometers at.” After the warm up, the treadmill speed was recorded and the natural running step rate of each participant was measured by a researcher visually counting the number of foot contacts in a thirty second period (with the participant running on the treadmill) and recording this as “steps per minute”. Participants next entered the anti-gravity treadmill set to the self-selected pace. After a sixty second familiarization period running at 100% of bodyweight, participants ran at nine randomized bodyweight intervals for sixty seconds each, ranging from 100% of BW to 20% of BW in 10% increments. Cadence was recorded for the final thirty seconds of each period. Part 2: The participant’s self-selected pace and natural running cadence was determined on the standard treadmill in the same manner described above. A cell phone metronome was used to audibly cue 100%, 105%, and 110% of natural cadence, and the participant performed the step rate for a sixty second period. Participants then entered the anti-gravity treadmill and ran at each of the nine randomized BW% conditions as described above. For each interval, participants again attempted to perform natural (100%) step rate, 5% increased, and 10% increased step rate, as cued by a metronome. If a participant was unable to sustain natural cadence at a given BW% interval, the increased step rate condition was not attempted for that body weight interval, and the tester instead transitioned the anti-gravity treadmill to the next randomized body weight condition. Similarly, if unsuccessful at a 5% cadence increase, a 10% cadence increase was not attempted.All participants gave their informed consent to participate, and the study was approved by the University of Minnesota Institutional Review Board. In order to statistically determine differences across body weight trials, a repeated measures ANOVA was used, as well as post-hoc t-tests. Statistical analysis was performed using IBM SPSS Statistics for Windows, v23 (IBM Corp., Armonk, NY). Significance was set at p<0.05.
RESULTS
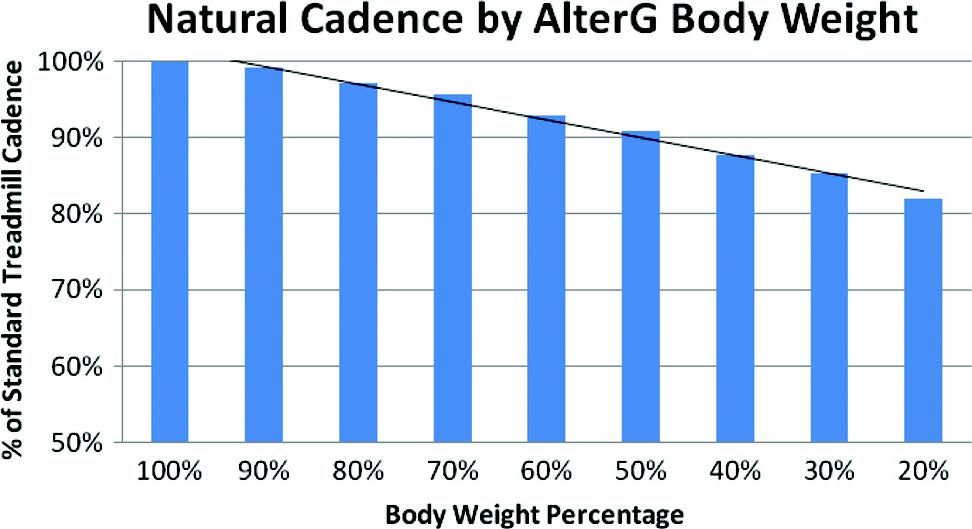
There were 30 participants (19 females and 11 males) with a mean age of 27.3 years old (range, 22-45 years old) in Part 1, and nine participants (2 females and 7 males) with a mean age of 29.6 years old (range, 25-40 years old) in Part 2. For Part 1, a repeated measures ANOVA showed a significant effect of natural running cadence on the anti-gravity treadmill at reduced body weight percentages (p<.01). Post-hoc t-tests revealed that every 10% bodyweight interval was significantly lower than the previous 10% interval (p<.01) on the anti-gravity treadmill, with cadence decreases ranging from 1.5%-3.5% between intervals (Figure 1). In relation to baseline cadence, the first 10% decrease in cadence occurred at roughly 50% of body weight, followed by a 20% decrease in cadence occurring at roughly 20% of body weight (Figure 1). For Part 2, seven of the nine participants were able to successfully perform baseline, 5% increase, and 10% increase in running cadence on both the standardtreadmill and for all nine body weight conditions on the anti-gravity treadmill. One participant was unable to sustain a 5% cadence increase at 60% of body weight, and was also unable to sustain a 10% cadence increase at 20% of body weight (which were the first two randomized BW conditions). However, this participant successfully completed the 5% and 10% increase in cadence conditions at all other body weight percentages. Another participant failed to perform 5% or 10% cadence increases at 20%, 30%, 50%, and 70% of body weight conditions, which were the final four randomized body weight levels, respectively.
DISCUSSION
The results of Part 1 indicate that natural step rate at any decreased BW% on an anti-gravity treadmill will be less than natural cadence on a standard treadmill at a self-selected, 5k pace. This is consistent with findings from previous studies performed at set speeds.18,21 While cadence data points were significantly different between each BW% levels, the values ranged from 1.5-3.5% between intervals, which may not be clinically relevant as previous literature has shown a significant change in muscle activation with a minimum cadence change of 5%.16 However, expecting a 10% decrease in cadence at 50% of body weight and a 20% decrease in cadence at 20% of body weight may be helpful for clinicians in prospectively estimating standard treadmill cadence based on anti-gravity treadmill performance. Additionally, these findings may assist clinicians in selecting a desirable bodyweight support level to minimize change in running cadence and to minimize the natural decrease in cadence with BW support for runners who aim to maintain a set cadence. Of note, this study was performed on a healthy population, and, if repeated on an injured population, a trend of anti-gravity treadmill natural step rate may be need to be ascertained for a specific rehab population.
Step rate manipulation of natural standard treadmill running cadence and 5% and 10% increases were successfully performed by 77.8% of participants. Two participants were unable to complete all cadence conditions. One of the two participants failed during the early-randomized BW% levels, yet successfully completed each condition at all other BW% intervals, suggesting a delayed learning effect of either an anti-gravity treadmill environment orwith matching the metronome cue. For the second participant, the failed attempts all appeared towards the end of data collection, perhaps due to a potential fatigue effect for this particular participant. The results of Part 2 provide evidence that, in a healthy, active population, cadence can be reproduced at natural step rate and up to 10% increased step rate on an anti-gravity treadmill, regardless of the body weight percentage experienced while running. The authors are currently unaware of any previously reported literature that either confirms or refutes these findings. This information may benefit runners who utilize the anti-gravity treadmill as a training modality and are attempting cadence manipulation. These results indicate that running cadence at any body weight level on an anti-gravity treadmill can be expected to be less than over-ground cadence. Compared to natural cadence on a standard treadmill, one can expect a 10% decrease in cadence at 50% bodyweight and a 20% decrease in cadence at 20% bodyweight. These values may be helpful for clinicians in forming expectations for over ground running cadence based on anti-gravity treadmill performance. Furthermore, this study lays a foundation for future investigations on injured runners, a population that may benefit from gait retraining in the early stages of the rehabilitation process. The anti-gravity treadmill offers potential for earlier initiation of cadence retraining, fostering neuromuscular adaptations prior to returning an injured athlete to over ground running. Utilizing an anti-gravity treadmill may also be desirable as a method of estimating over ground running cadence in injured runners training on an antigravity treadmill at their current level of function. Knowing the expected reduction in cadence that naturally occurs as body weight support increases can allow clinicians to gauge the progress of their patient in reaching their natural cadence based upon the level of body weight support is being utilized. There are several limitations of this study. First, it was performed on a healthy population, with the understanding that if repeated on an injured population, a different trend of anti-gravity treadmill cadence may be realized. Second, having novicerunners self-select their speed may alter the ability to manipulate cadence, as faster speeds may put more demand on running mechanics as well as the cardiovascular system as a whole. A further limitation of the study is potential for error in data collection due to the researcher visually counting foot strikes as compared to objective data collection with pressure sensors used in past studies. However, the results of this current study are consistent with the past studies, which supports visual tracking of cadence as a convenient alternative to more costly methods.
CONCLUSION
Running at decreased BW% on an anti-gravity treadmill yields a significant and linear decrease in cadence when performed at a self-selected, moderate intensity pace, as compared to cadence on a standard treadmill. On an anti-gravity treadmill, each 10% decrease in body weight resulted in a significant decrease in natural running cadence. Further, the vast majority of healthy individuals are able to maintain and increase their natural cadence at varying body weight percentages, which supports the possibility of cadence training taking place prior to injured individuals commencing full body weight running. The appropriate cadence manipulation candidate may benefit from earlier initiation of cadence retraining, and this may be possible in the reduced bodyweight environment that the antigravity treadmill provides.